위암 수술 후 장마비에 대한 한의학적 치료의 효과 : 체계적 문헌 고찰 및 메타분석
The Effectiveness of Traditional Korean Medicine for Treating Postoperative Ileus in Gastric Cancer Patients: A Systematic Review and Meta-Analysis
Article information
Trans Abstract
Objectives:
Postoperative ileus (POI) is a common impairment of gastrointestinal motility and causes a delay in postoperative recovery, as well as an increased length of hospital stay, but no single strategy has a significant recuperative effect on POI. Studies of traditional Korean medicine (TKM) have reported improvements in bowel function after surgery. The aim of this systematic review was to assess the effectiveness of TKM on postoperative ileus in gastric cancer patients.
Methods:
We used six databases to search for studies published from January 1, 2007, until May 11, 2022. The included studies were those reporting gastric cancer patients who received TKM treatment after gastrectomy through indicators related to POI.
Results:
The search identified 27 RCTs that used herbal medicine (Daegeonjung-tang and Gami-leejoongtang), herbal medicine combined with acupuncture (Sama-tang, Gumiseunggi-tang, Daeseunggi-tang, and Insam-tang), acupuncture, acupuncture and moxibustion, electroacupuncture, warm needling, transcutaneous electroacupuncture (TEA), low-frequency electrical acupoint stimulation (LEAS), moxibustion, auricular acupressure, and ST-36 acupoint injection with neostigmine as treatments for POI. The time to first flatus was shortened by herbal medicine combined with warm needling (Sama-tang, Gumiseunggi-tang, Daeseunggi-tang, and Insam-tang), acupuncture, electroacupuncture, warm needling, TEA, moxibustion, auricular acupressure, and ST-36 acupoint injection with neostigmine (p<0.00001). The time to the first defecation decreased significantly in response to the herbal medicine combined with warm needling (Sama-tang, Gumiseunggi-tang, Daeseunggi-tang, and Insam-tang), acupuncture, electroacupuncture, warm needling, TEA, moxibustion, auricular acupressure, and ST-36 acupoint injection with neostigmine (p<0.00001). No serious adverse events occurred.
Conclusions:
TKM could be a promising option for preventing and resolving POI in gastric cancer patients after gastrectomy.
Abstract
목적:
본 연구는 위암 수술 후 장마비의 한의학적 치료 효과를 평가하기 위해 수행하였다.
방법:
2007년 1월 1일부터 2022년 5월 11일까지 출판된 연구들을 6개의 데이터베이스를 통해 수집하였다. 수술 후 한의학적 치료를 받은 위암 환자를 장마비 관련 지표들을 통해 관찰한 연구들을 선정하였다.
결과:
한약, 침, 뜸, 전기혈위자극, 이혈요법, 족삼리혈의 약물 주입을 수술 후 장마비 치료법으로 사용한 27편의 연구를 선정하였다. 한약, 한약과 침 병용요법, 침, 뜸, 전기혈위자극, 이혈요법, 족삼리혈의 네오스티그민 주입 치료군에서 수술 후 첫 가스 배출까지의 시간이 감소하였고 (p<0.00001), 수술 후 첫 배변까지의 시간이 한약. 한약과 침 병용요법, 침, 뜸, 전기혈위자극, 이혈요법, 족삼리혈의 네오스티그민 주입 치료군에서 유의미하게 감소하였다 (p<0.00001). 심각한 이상반응은 나타나지 않았다.
결론:
한의학적 치료는 위절제술 후 위암 환자에게 수술 후 장마비의 예방과 치료법으로 활용될 수 있으며 수술 후 장마비 치료의 임상적 효과를 명확히 하기 위해 후속 연구가 필요하다.
I. Introduction
Gastric cancer is the fifth most common cancer and the fourth leading cause of cancer deaths worldwide in 20201. The most recommended treatment is radical gastrectomy with lymph node dissection for patients with resectable early gastric cancer, as patients have improved survival after complete resection. Nevertheless, patients typically have a relatively slow postoperative recovery after gastrectomy, resulting in decreased survival and an increased length of hospital stay2-4.
Postoperative ileus (POI) is transient impairment of gastrointestinal motility lasting 3-5 days after surgery. It is characterized by nausea, vomiting, bloating, abdominal pain, loss of bowel movement, and the inability to pass flatus5. When this dysfunction lasts beyond the expected time, it is called “paralytic” or “prolonged” postoperative ileus (PPOI)6,7. Preventing POI is important to shorten the postoperative recovery period after gastrectomy8 because PPOI is one of the main factors for a delay in postoperative recovery9,10. The most commonly used clinical criteria to assess the resolution of POI are passage of flatus and stool, tolerance of an oral diet, and the presence of bowel sounds, so the primary therapeutic target in patients with POI is to shorten the time to first flatus and defecation7.
As POI is a major obstacle to rapid recovery after abdominal surgery, including gastrectomy, pharmacological and nonpharmacological treatments have been attempted, but have been proven to be either ineffective or minimally effective11,12.
Traditional Korean medicine (TKM) treatment is becoming a promising option to treat POI. TKM treatments, including acupuncture, acupressure, and herbal medicines, have a positive effect on the recovery of bowel function in cancer patients13-15. However, comprehensive research on the effect of TKM treatment on POI in gastric cancer patients has not been conducted. Therefore, we conducted a systematic review and meta-analysis to assess the effectiveness of TKM in improving bowel function and preventing or treating POI in gastric cancer patients.
II. Methods
1. Inclusion and exclusion criteria
1) Types of study
We included all prospective randomized clinical trials (RCTs) available across the six databases (PubMed, the Cochrane Library, RISS, KISS, CNKI, and J-STAGE) selected. We excluded case studies, case series, and retrospective clinical studies.
2) Types of participant
We included gastric cancer patients after surgery.
3) Types of intervention
We included studies using Traditional Korean Medicine (herbal medicine, moxibustion, acupuncture, electro-acupuncture), regardless of the combination of Western medicine. The inclusion criteria for the controls were no treatment, placebos, or conventional medicines.
4) Types of outcome measure
The data of studies could be pooled for time to first flatus (twenty-six studies), time to the first defecation (twenty-one studies), the incidence of postoperative ileus (three studies), and adverse events (nine studies).
(1) Primary outcomes: time to first flatus, time to the first defecation
(2) Secondary outcomes: incidence of postoperative ileus, adverse events
2. Search methods
1) Searched electronic databases
We used six databases to search for limited languages in English, Japanese, Chinese, and Korean among the studies published from Jan 1, 2007, until May 11, 2022. The databases included were PubMed, the Cochrane Library, two Korean medical databases (the Research Information Service System[RISS], the Korean Studies Information Service System[KISS]), one Chinese medical database (China National Knowledge Infrastructure[CNKI]), and one Japanese medical database(Japan Science Technology Information Aggregator, Electronic [J-STAGE]).
2) Search strategy
The search terms we used were ‘gastric cancer’ OR ‘gastric neoplasm’ OR ‘gastric adenocarcinoma’ OR ‘stomach cancer’ OR ‘stomach neoplasm’ OR ‘stomach neoplasms’ OR ‘gastrectomy’ AND postoperative OR postsurgical OR ileus OR gastroparesis OR ‘gastrointestinal function’ OR ‘gastrointestinal motility function’ OR surgery AND ‘herbal medicine’ OR ‘Korean medicine’ OR ‘Chinese medicine’ OR moxibustion OR acupuncture OR herb OR plant OR ‘auricular pressure’ OR ‘auricular acupressure’. The search strategy involved using a mixture of the search terms in Korean and Chinese.
3. Selection of studies and data extraction
Two reviewers (HRB, EJK) selected potentially eligible articles by reading through titles and abstracts. These reviewers examined hard copies of the publications to determine their suitability. Any disagreements were resolved through discussion, and where necessary, in consultation with a third reviewer (NHL).
Two reviewers (HRB, EJK) extracted data from the studies included. Information that was excluded was as follows; the characteristics of subjects, the outcomes, and the results. We resolved disagreements through discussion and in consultation with the third author (NHL), who acted as an arbiter.
4. Assessment of risk of bias
Two reviewers (HRB, EJK) independently evaluated the risk of bias (ROB) in the studies included by following the guidelines given in the “Cochrane Handbook of Systematic Reviews of Interventions (i.e., sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting)”.
5. Data synthesis
We presented dichotomous data in terms of risk ratios, with 95% confidence intervals (CIs). The mean difference with 95% CIs for continuous data is used in this study.
The Review Manager 5.4.1, the Cochrane Collaboration’s software program, was used to perform the statistical analysis. We used weighted mean differences (WMD) with 95% confidence intervals (CIs) for calculating continuous data, and I2 test for assessing the heterogeneity of the data. If heterogeneity existed (I2≥50%), a random-effects model was applied. If or not, a fixed-effects model was applied. Statistically significant difference was considered as p<0.05.
III. Results
1. Study description
Of 76 eligible study hits, twenty-six studies were excluded after duplicates were removed. After assessing the fifty abstracts of the studies, twenty studies are excluded. After assessing the thirty full-text articles, three studies were excluded for various reasons (Fig. 1). Finally, twenty-seven studies met our inclusion criteria16-42. Summaries of the key data from these studies are shown in Table 1. Of the twenty-seven studies, one trial was conducted in Korea19, two were performed in Japan18,20, and twenty-four were conducted in China16,17,21-42. Twenty-five studies included gastric cancer patients after gastrectomy (laparoscopic gastrectomy29,37, total gastrectomy20,24, open total gastrectomy18, distal gastrectomy19,42, or total or partial gastrectomy17,21-23,25-27,30-36,38-40,41), one study was undertaken with gastric cancer patients diagnosed with PPOI following gastrectomy16, and the other one study was conducted for abdominal distension patients after gastrectomy28. Test interventions included Daegeonjung-tang (Daikenchuto; DKT, Da-Jian-Zhong-Tang) (two studies), Gami-leejoongtang (modified Lizhong tang) (one study), Sama-tang (Simotang) combined with warm needling (two studies), Gumiseunggi-tang (Jiuwei Chengqi Oral Liquid) combined with warm needling (one study), Daeseunggi-tang (Dachengqi decoction) combined with warm needling (one study), Insam-tang (Renshen decoction) combined with acupuncture (one study), acupuncture (three studies), acupuncture and moxibustion (one study), warm needling (two studies), electroacupuncture (one study), transcutaneous electroacupuncture (TEA) (one study), transcutaneous electrical acupoint stimulation (TEAS) (one study), low-frequency electrical acupoint stimulation (LEAS) (one study), acupoint injection with neostigmine (one study), and moxibustion (four studies), and auricular acupressure (four studies).

Flow chart of study selection process.
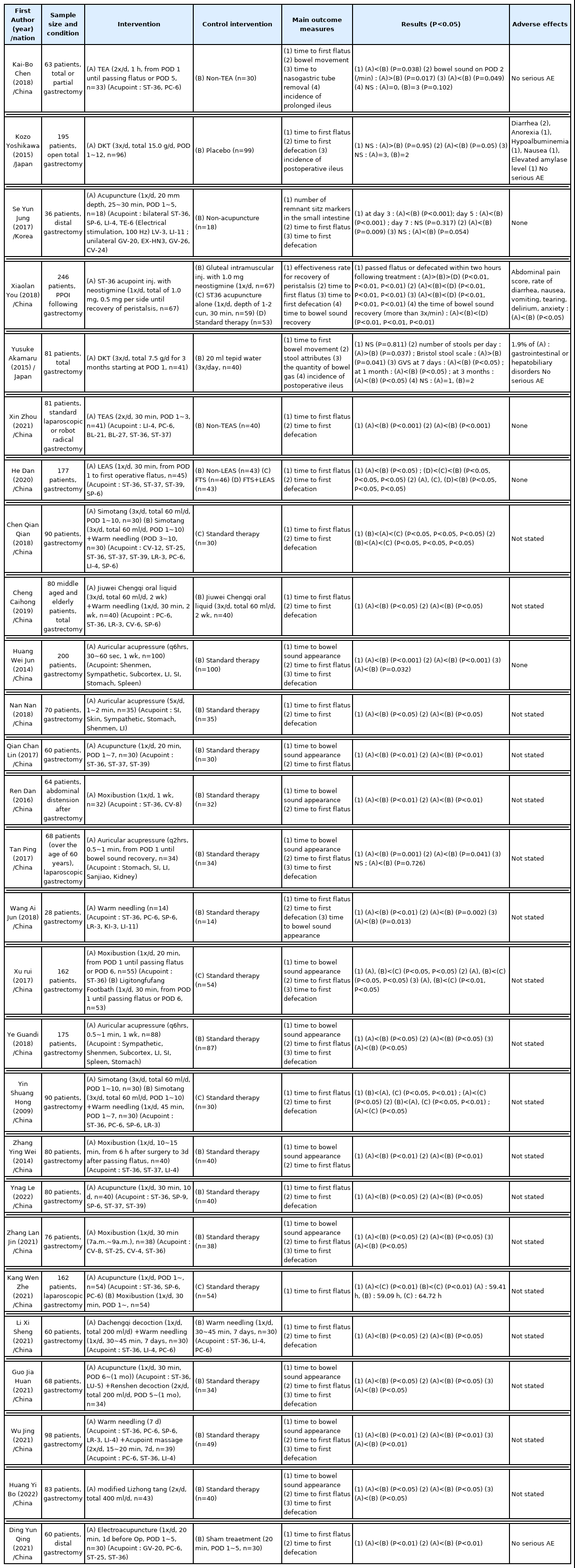
Summary of included Randomized Clinical Trials
2. Risk of bias
1) Random sequence generation
Sixteen studies reported using a random sequence generation method, and we rated random sequence generation as a low risk of bias16,17,21,22,25-27,29,32,34,35,38,39,40-42. We rated the other eleven studies as having an unclear risk of bias because no randomization methods were described.
2) Allocation concealment
Allocation concealment was not described in any of the studies, and we rated the risk of bias as unclear.
3) Blinding of participants and personnel
Only two studies conducted double-blind trials by comparing the treatment groups with placebo groups; we rated these studies as having a low risk of bias18,42. In the five trials, because the participants were not blinded, we rated them as having a high risk of performance bias16,17,19-21. One of these studies reported that no blinding was applied to participants or physicians because the treatments had different characteristics16. In the remaining trials, we rated them as having an unclear risk of performance bias because there was no statement about the blinding of participants.
4) Blinding of outcome assessment
The method for blinding outcome assessors was not reported for twenty-six trials, so we rated them as having an unclear risk of detection bias. We rated one study that reported outcome assessor blinding as having a low risk of detection bias16.
5) Incomplete outcome data
Four studies reported the reasons for discontinuing the intervention, and we rated these as having a low risk of bias16,18-20. The other studies had an unclear risk of attrition bias because they did not report dropout cases.
6) Selective reporting
One study predefined the outcomes and demonstrated all predefined measurements. We rated that study as having a low risk of reporting bias19. We rated the other trials as having an unclear risk of reporting bias because they did not report whether the study was registered or whether the study protocol was publicly assessable.

Risk of bias.

Risk of bias summary.
7) Other bias
Because of insufficient information to judge, we rated all of the studies as having an unclear risk of reporting bias.
3. Outcomes
1) Time to first flatus
Twenty-six studies reported data on time to the first flatus. There was a significant decrease in time to first flatus in the studies of Gami-leejoongtang41, Sama-tang combined with warm needling23,33, Gumiseunggi-tang combined with warm needling24, Daeseunggi-tang combined with warm needling38, Insam-tang combined with acupuncture39, acupuncture19,27,35, acupuncture and moxibustion37, electroacupuncture42, warm needling30,40, TEA17, TEAS21, LEAS22, ST-36 acupoint injection with neostigmine16, moxibustion28,31,34,36, and auricular acupressure25,26,29,32.
Meta-analysis results revealed significant decreases in the time to first flatus in the acupoint stimulation studies (MD=-15.62, 95% CI : -18.98 to -12.26, I2=96%) (Fig. 4).

Forest plot of acupoint stimulation group versus control group: time to first flatus.
The TEA, TEAS, LEAS, and electroacupuncture study showed that the time to first flatus following surgery was significantly shorter in the TEA, TEAS, LEAS, and electroacupuncture groups than in the non-treatment groups17,21,22,42 (p=0.038, p<0.001, p<0.05, p<0.01). The time to first flatus in the acupuncture trials was significantly shorter in the acupuncture groups than that in the non-acupuncture groups19,27,35 (p=0.009, p<0.01, p<0.05). A significant decrease in the time to first flatus was reported in the treatment groups in the auricular acupressure studies25,26,29,32, compared with the non-treatment groups (p<0.001, p<0.05, p=0.041, p<0.05). The time to first flatus in the Gami-leejoongtang trial was significantly shorter in the Gami-leejoongtang group than that in the non-treatment group41 (p<0.05).
In the warm needling studies30,40, the time to first flatus after gastrectomy was shorter in the warm needling groups than in the non-treatment groups (p<0.01, p<0.01). The Sama-tang combined with warm needling studies reported that the time to first flatus was shorter in the Sama-tang combined with warm needling groups than in the non-treatment groups23,33 (p<0.05, p<0.01). In the Gumiseunggi-tang combined with warm needling study, the time to first flatus following surgery was shorter in the Gumiseunggi-tang combined with warm needling group than in the Gumiseunggi-tang group24 (p<0.05). The Daeseunggi-tang combined with warm needling study showed that the time to first flatus was shorter in the Daeseunggi-tang combined with warm needling group than in the warm needling group38 (p<0.05). In the Insam-tang combined with acupuncture study39, the time to first flatus was shorter in the treatment group than in the non-treatment group (p<0.05).
The ST-36 acupoint injection study reported a significantly shorter time to first flatus in the ST-36 acupoint injection group than that in the standard therapy group, but it was not significantly shorter in the acupuncture group than in the standard therapy group (p=0.175). In this study, standard therapy was gradual ambulation with simple exercises, fasting, intravenous fluids, and parenteral nutrition16. The moxibustion studies28,31,34,36 showed that the time to first flatus was shorter in the moxibustion groups than in the non-treatment groups (p<0.01, p<0.05, p<0.01, p<0.05). In the acupuncture and moxibustion study37, the time to first flatus was shorter in the acupuncture group and moxibustion group than in the non-treatment group (p<0.01, p<0.01).
In the DKT study18, the median time from the end of the operation (tracheal tube extubation) to the first flatus was slightly longer in the DKT group (68.9 h) than in the placebo group (68.3 h), but it was not significant.
2) Time to the first defecation
Twenty-one studies reported data on time to the first defecation. There was a significant decrease in time to the first defecation in the studies of Gami-leejoongtang41, DKT18, Sama-tang combined with warm needling23,33, Gumiseunggi-tang combined with warm needling24, Daeseunggi-tang combined with warm needling38, Insam-tang combined with acupuncture39, acupuncture35, electroacupuncture42, warm needling30,40, TEAS21, LEAS22, ST-36 acupoint injection with neostigmine16, moxibustion31,36, and auricular acupressure25,26,32.
Meta-analysis results revealed significant decreases in the time to the first defecation in the acupoint stimulation studies (MD=-16.26, 95% CI : -19.66 to -12.86, I2=97%) (Fig. 5).

Forest plot of acupoint stimulation group versus control group: time to first defecation.
The TEAS, LEAS, and electroacupuncture trial showed that the time to the first defecation was shorter in the TEAS, LEAS, and electroacupuncture groups than in the non-treatment groups21,22,42 (p<0.001, p<0.05, p<0.01). A significant decrease in the time to the first defecation was observed in the treatment groups in the Sama-tang combined with warm needling studies, compared with the non-treatment groups23,33 (p<0.05, p<0.01). In the Gumiseunggi-tang combined with warm needling study, the time to the first defecation was significantly shorter in the Gumiseunggi-tang combined with warm needling group than in the Gumiseunggi-tang group24 (p<0.05). The Daeseunggi-tang combined with warm needling study showed that the time to the first defecation was shorter in the Daeseunggi-tang combined with warm needling group than in the warm needling group38 (p<0.05). A significant decrease in the time to the first defecation was reported in the treatment group in the Insam-tang combined with acupuncture trial, compared with the non-treatment group39 (p<0.05).
A significant decrease in the time to the first defecation was observed in the treatment group in the DKT study (94.7 h), compared with the placebo (113.9 h) (p=0.05)18. In the Gami-leejoongtang study, the time to the first defecation was shorter in the Gami-leejoongtang group, compared with the non-treatment group41 (p<0.05). The acupuncture trials reported that the acupuncture groups had a relatively faster time to first defecation (p=0.054, p<0.05)19,35. In the auricular acupressure trials, the time to the first defecation was shorter in the treatment groups, compared with the non-treatment groups25,26,29,32 (p=0.032, p<0.05, p=0.726, p<0.05).
In the ST-36 acupoint injection with neostigmine study, the time to the first defecation was significantly shorter in the acupoint injection group than that in the standard therapy group (p<0.01), but it was not significantly shorter in the acupuncture group than the standard therapy group (p=0.256)16. The warm needling trials reported that the time to the first defecation was shorter in the warm needling groups than in the non-treatment groups30,40 (p=0.002, p<0.01). A decrease in the time to the first defecation was reported in the treatment groups in the moxibustion trials, compared with the non-treatment groups31,36 (p<0.05, p<0.05).
3) Incidence of postoperative ileus
Three of 96 patients in the DKT group and two of 99 patients in the placebo group presented with POI in a study by Kozo Yoshikawa18. One of 51 patients in the DKT group and two of 40 patients in the placebo group developed an intestinal obstruction within 3 months in a study by Yuseke Akamaru20. There was no statistical difference in the incidence of POI between treatment groups and control groups from the above-mentioned RCTs using DKT. The TEA trial reported that the incidence of prolonged ileus was 0 in the TEA group and 3 in the non-TEA group (p=0.102), with prolonged POI defined in this study as not passing flatus for 5 days after the gastrectomy.
4) Adverse events
No serious adverse events were reported in any of the included RCTs.
IV. Discussion
Surgical treatment is recommended for gastric cancer patients, most of whom suffer from functional gastrointestinal disorders during the postoperative period. Although POI is common, inhibits early recovery, and increases the length of hospital stay, there is no exact etiology or treatment for POI. Several TKM treatment studies have reported that TKM improves bowel function after surgery. We conducted a systematic review and meta-analysis of the effectiveness of TKM treatment for POI in gastric cancer patients.
The time to first flatus in gastric cancer patients after gastrectomy was shortened by the TKM treatments, such as herbal medicine combined with acupuncture (Sama-tang, Gumiseunggi-tang, Daeseunggi -tang, Insam-tang), acupuncture, warm needling, moxibustion, auricular acupressure, TEAS, LEAS, TEA, electroacupuncture, and the acupoint injection (ST-36), which was demonstrated by the meta-analysis in this systematic review (Fig. 4). The time to the first defecation decreased significantly in response to herbal medicine combined with acupuncture (Sama-tang, Gumiseunggi-tang, Daeseunggi-tang, Insam-tang), acupuncture, warm needling, TEAS, LEAS, electroacupuncture, moxibustion, auricular acupressure, and the acupoint injection (ST-36) (Fig. 5).
POI is believed to be mediated by many factors, including gastrointestinal motility, the autonomic nervous system, neurotransmitters, local factors, hormones, and inflammation, which control bowel motility43. Thus, the complex interplay between these factors makes it difficult to understand the clear pathogenesis and determine an exact treatment for POI44.
The typically recommended approaches to alleviate POI include a nasogastric tube, early postoperative feeding, gum chewing, laparoscopic procedures, and pharmacological agents43,44. However, until now, no single strategy has had a significant effect on POI45. Thus, establishing a novel strategy to manage POI in patients with gastric cancer is important.
Acupuncture can directly restore gastrointestinal transit via the parasympathetic efferent pathway13,46. In addition, acupuncture increases postoperative bowel motility by activating the interstitial cells of Cajal (ICCs)47,48. ICCs, the pacemaker cells of gastrointestinal motility, generate and propagate slow electrical waves and act as mediators that transmit enteric neural input to smooth muscle cells49.
Recent studies47,50 have demonstrated that electroacupuncture (EA) decreases intestinal inflammation, which is the main factor associated with delayed dysfunction of the gastrointestinal tract51. EA activates the 7nAChR-mediated Janus kinase 2/signal transducer and activator of transcription 3 (JAK2/STAT3) signaling pathway in POI.
DKT is a traditional herbal medicine composed of dried pepper, processed ginger, ginseng radix, and maltose powder18. DKT has been used to treat gastrointestinal disorders, including adhesive ileus and paralytic ileus52-58. DKT has been recently reported to significantly inhibit cyclooxygenase-2 activity59 and downregulate various inflammatory mediators, including tumor necrosis factor-α, interleukin-1β, and endothelin-1. Mechanistic studies on the TKM treatments mentioned above are thought to lay the theoretical foundation for the RCT results included in this systematic review.
This study had some limitations. The first limitation is that except two studies18,42, the majority of the trials were not blinded to the physicians and participants or there was no statement about blinding, which is related to preventing bias because of the demanding characteristics or placebo effects. Furthermore, the databases considered in this study were limited to English, Japanese, Chinese, and Korean literature, which may have contributed to bias.
In conclusion, this study suggests that acupuncture, TEA, TEAS, LEAS, electroacupuncture, DKT, Gami-leejoongtang, Sama-tang combined with warm needling, Gumiseunggi-tang combined with warm needling, Daeseunggi-tang combined with warm needling, Insam-tang combined with acupuncture, warm needling, moxibustion, auricular acupressure, and acupoint injection with neostigmine improved the gastrointestinal function of gastric cancer patients after gastrectomy during the postoperative recovery period compared with control interventions. Thus, TKM should be considered a promising option for preventing and resolving POI in gastric cancer patients. Further well-designed studies are needed to clarify these findings and determine better interventions for POI.
Acknowledgement
This research was supported by the Daejeon University fund (2021).