Park, Lee, and Bae: Cold Hypersensitivity and Sleep Quality: A Cross-sectional Community-based Study
Abstract
Background:
Cold hypersensitivity (CH) and sleep disorders are not limited to patients with specific diseases, as they are also commonly observed in the general population. The objective of this study was to investigate the relationship between CH and sleep quality.
Methods:
This cross-sectional study analyzed data from a cohort of 5,052 individuals living in South Korea. Based on the results of a questionnaire on CH, the participants were classified into four groups: non-CH, CH in the hands (CHH), CH in the feet (CHF), and CH in the hands and feet (CHHF). Sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI). Multiple regression was used for groupwise comparisons of total PSQI scores and the scores for each component, and logistic regression was used to find the odds ratios of being a “poor sleeper” (PSQI≥8.5).
Results:
The CHF and CHHF groups showed significantly higher scores than the non-CH group on the overall PSQI as well as on the following sleep components: subjective sleep quality, sleep latency, habitual sleep efficiency, sleep disturbance, and sleep medication use. The odds ratios for being a “poor sleeper” were significant in the CHF (1.84; CI=1.38-2.43) and CHHF groups (1.54; CI=1.25-1.89), but the CHH group did not show any difference from the non-CH group. We identified a correlation between CH in the feet and poor sleep quality.
Conclusions:
These findings help to elucidate the relationship between sleep and CH and highlight the need to clarify the underlying mechanism.
KeywordsKeywords: cold extremities, cold feet, cold hypersensitivity, insomnia, Pittsburgh sleep quality index
I. Introduction
Although the function of sleep remains unclear, it is known to be involved in restoration of the body and the immune function 1, thermoregulation 2, and removal of waste products from the brain 3, making it essential for sustaining human life and function. However, in modern times, many people suffer from insomnia or other sleep disorders, and the number of patients is increasing. A population-based cohort study in the United States that followed-up 1,246 adults found an incidence of chronic insomnia of 9.3% 4. A large cross-sectional study in Norway with 40,535 respondents found an incidence of insomnia of 7.1% 5. A Korean study of 881 elderly individuals aged 60 years or older reported an incidence of insomnia of 32.8% 6, and data published by the Korean National Health Insurance Service showed that the number of patients receiving treatment for sleep disorders increased from 420,000 in 2014 to 570,000 in 2018, an average annual increase of 8.1% 7. Although there are some discrepancies between these studies, sleep complaints (e.g., difficulty falling asleep, sleep continuity disturbance, insomnia) are generally known to be more prevalent in females ,5 the elderly 8, and obese individuals 4. In addition, psychiatric and physical disorders such as depression, cardiac disease, diabetes, migraine, fatigue, and cold hypersensitivity (CH) in the hands and feet (CHHF) have also been reported to cause, exacerbate, or accompany sleep disorders 4,9-12. CHHF refers to the condition of feeling excessive coldness of the hands and feet in situations where people do not typically feel cold, to the extent that the individual feels discomfort in their daily life 13,14. This condition also shares similarities with “hie-sho” (Japanese) ,10 cold constitution 15, cold extremities ,12 and primary vascular dysregulation 16. These symptoms are known to be more common among Asians, women, and lean individuals. Although the results have not always been consistent between different investigations, these symptoms are estimated to be present in 30% of women and 10% of men 12,14. In Korean medicine, sleep disorders can arise from a yin-yang disharmony (陰陽失調), resulting in a nutrient-defense disharmony (營衛不和). In such cases, the body may present with patterns of yin deficiency (陰虛) and heat syndrome (熱證), or yang deficiency (陽虛) and cold syndrome (寒證) 17. A representative symptom associated with these patterns is an excessive sense of cold or heat, with CHHF being particularly prevalent 14. Given the high prevalence of CH and sleep disorders, as well as the approach of traditional Korean medicine to sleep disorders, it is considered worthwhile to investigate the relationship between sleep quality and cold hands and feet in depth. One study of 238 Japanese women reported that women with cold extremities had significantly higher Pittsburgh Sleep Quality Index (PSQI) scores 9. In a study of 2,800 Swiss citizens aged 20-40 years, individuals with thermal discomfort from cold extremities had more than twice as many difficulties initiating sleep as those without thermal discomfort 12. Finally, a study that compared 32 patients with primary vasospastic syndrome to 31 healthy controls found that the patients had a significantly more prolonged sleep-onset latency 18. Despite these findings, there have been few studies on CH and sleep disorders in a sample including both sexes and diverse age groups. Therefore, in this study, we examined a cohort of residents from two regions in Gyeonggi-do, South Korea, with the aim of (a) investigating the relationship between CH and sleep status using the CH questionnaire and the PSQI and (b) analyzing whether there were any differences among the PSQI components in persons with vs. without CH.
II. Methods
1. Data collection
This was a cross-sectional study. Data were obtained from the Korean Medicine Data Center (KDC) for 5,787 persons from two regions in Gyeonggi-do, South Korea 19,20. The data had been collected between 2012 and 2015. This is a cohort, population-based study conducted as part of “The Korean Genome and Epidemiology Study (KoGES)”, and has been conducted to date in the Anseong and Ansan regions in Gyeonggi-do, South Korea, under the name of “KoGES_Ansan and Ansung study”. Additionally, the KDC collected questionnaires based on Korean medicine (e.g., Sasang constitution, pattern identification), blood tests, and body measurements from the 2013-2015 participants, which were also analyzed in the present study. This study was approved by the Institutional Review Board of the Korea Institute of Oriental Medicine (I-0910/02-001).
2. PSQI
The state of participants’ sleep quality was measured using the Korean version of the PSQI questionnaire. The PSQI is a self-report used to assess the state of sleep in the previous month and is one of the main instruments used for this purpose 21. The questionnaire consists of seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction. Each component was scored on a scale of 0-3 points, and the sum of the seven components was the total PSQI score. Higher scores indicate poorer sleep quality. In the original version of the PSQI, the cut-off value to differentiate between “good sleepers” and “poor sleepers” is >5 points 21. However, based on a study by Sohn, which used the Korean translation of the PSQI questionnaire 22, we defined “poor sleepers” as participants with a score ≥8.5 because all the participants in the present study were Korean.
3. CH status
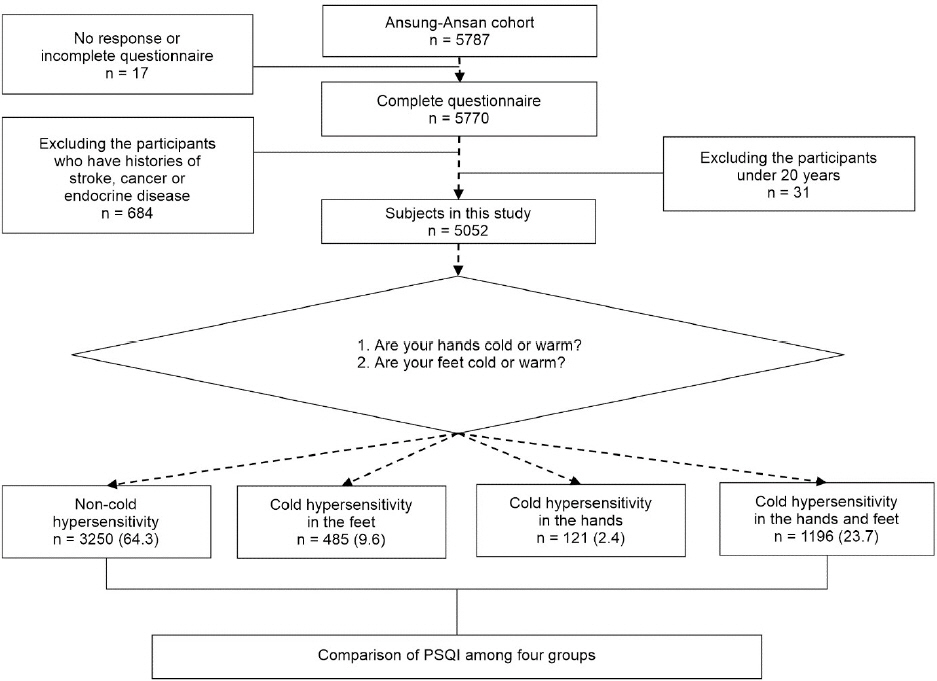
CH was identified by asking the participants two simple questions about the sensation in their hands and feet in the last 6 months (“Are your hands cold or warm?” and “Are your feet cold or warm?”). Participants who responded “warm” or “intermediate” for the hands and feet were placed in the Non-cold hypersensitivity (Non-CH) group; participants who responded “cold” for their hands but “warm” or “intermediate” for their feet were placed in the CH in the hands (CHH) group; participants who responded “cold” for their feet but “warm” or “intermediate” for their hands were placed in the CH in the feet (CHF) group; finally, participants who responded “cold” for both their hands and feet were placed in the CHHF group ( Fig. 1).
Fig. 1
Flow chart of the study.
Non-cold hypersensitivity : the group of participants who responded “warm” or “intermediate” to Questions 1 and 2; cold hypersensitivity in the feet : the group of participants who responded “warm” or “intermediate” to Question 1 and “cold” to Question 2; cold hypersensitivity in the hands : the group of participants who responded “cold” to Question 1 and “warm” or “intermediate” to Question 2; cold hypersensitivity in the hands and feet : the group of participants who responded “cold” to Questions 1 and 2.
4. Anthropometric measurements and blood pressure
Neck circumference was measured at the inferior margin of the thyroid cartilage (cricothyroid membrane), with the participant seated. Waist circumference was measured horizontally through the navel, with the participant standing. Height and body weight were measured directly, and body temperature was measured from the tympanic membrane. Blood pressure was measured using a mercury sphygmomanometer on the left upper arm. Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg, in accordance with the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure 23. Hypotension does not fit any disease concept and there are no standards of normality, but it is known to accompany cold extremities. In the present study, hypotension was defined as systolic blood pressure ≤100 mmHg or diastolic blood pressure ≤60 10,24.
5. Sasang constitution
The Sasang constitutional types were classified using the Korea Sasang Constitutional Diagnostic Questionnaire (KS-15). This questionnaire can distinguish Taeeum-in, Soyang-in, and Soeum-in types, excluding the Taeyang-in type. The questionnaire includes items on body mass index (BMI), personality, and ordinary symptoms 25.
6. Statistical methods
The general characteristics of the participants are provided as the mean, standard deviation, frequency, and percentage, and differences were analyzed using analysis of variance (ANOVA) or chi-square tests. PSQI scores were compared between groups using ANOVA, with Scheffé’s method for post-hoc testing. Multiple regression was used to compare differences between groups while correcting for sex, age, BMI, body temperature, blood pressure, neck and waist circumference, and sociodemographic variables. A chi-square test was used to compare the frequencies of “poor sleepers”, and logistic regression was used to obtain the odds ratio and 95% confidence interval of being a “poor sleeper” in each of the CH groups compared with the Non-CH group. The statistical significance level was set at p<0.05. Statistical analysis was performed using SPSS software (version 24.0; IBM Corp., Armonk, NY, USA).
III. Results
1. Demographic characteristics
In total, the data of 5,052 participants were used in the analysis, and the mean age was 62.3±9.2 years, with 2,425 males (48.0%) and 2,637 females (52%). The proportion of males in the Non-CH and CHH groups was higher, at 54.3% and 58.7%, respectively, while the ratio of females in the CHF and CHHF groups was higher, at 62.5% and 65.9%, respectively. Significant differences were observed between the groups for age, sex, marital status, education, tobacco use, alcohol consumption, blood pressure, BMI, body temperature, neck and waist circumference, and Sasang constitution, but not for hypertension ( Table 1).
Table 1
Characteristics of Participants Based on CH
|
Non-CH* (n=3,250) |
CHF† (n=485) |
CHH‡ (n=121) |
CHHF§ (n=1,196) |
P value |
|
Age |
62.5±8.7 |
60.4±9.8 |
62.4±8.1 |
62.8±10.3 |
<0.001 |
|
Gender |
Male |
1,764 (54.3) |
182 (37.5) |
71 (58.7) |
408 (34.1) |
<0.001 |
|
Female |
1,486 (45.7) |
303 (62.5) |
50 (41.3) |
788 (65.9) |
|
Marital status |
Spouseless |
441 (13.6) |
76 (15.7) |
16 (13.2) |
216 (18.1) |
0.002 |
|
Married |
2,809 (86.4) |
409 (84.3) |
105 (86.8) |
980 (81.9) |
|
Education |
≤Elementary |
1,109 (34.1) |
134 (27.6) |
38 (31.4) |
471 (39.4) |
<0.001 |
|
Middle, High |
1,648 (50.7) |
263 (54.2) |
65 (53.7) |
592 (49.5) |
|
≥College |
493 (15.2) |
88 (18.1) |
18 (14.9) |
133 (11.1) |
|
Tobacco |
No |
2,749 (84.6) |
439 (90.5) |
104 (86.0) |
1,071 (89.5) |
<0.001 |
|
Yes |
501 (15.4) |
46 (9.5) |
17 (14.0) |
125 (10.5) |
|
Alcohol |
No |
1,719 (52.9) |
294 (60.6) |
68 (56.2) |
746 (62.4) |
<0.001 |
|
Yes |
1,531 (47.1) |
191 (39.4) |
53 (43.8) |
450 (37.6) |
|
Systolic blood pressure |
121.6±16.2 |
120.3±17.5 |
121.1±16.5 |
119.6±18.1 |
0.005 |
|
Diastolic blood pressure |
77.1±10.0 |
76.9±10.7 |
77.7±9.8 |
75.0±10.3 |
<0.001 |
|
Hypertension |
No |
1,645 (50.6) |
284 (58.6) |
64 (52.9) |
701 (58.6) |
0.168 |
|
Yes |
1,605 (49.4) |
201 (41.4) |
57 (47.1) |
495 (41.4) |
|
Hypotension |
No |
2,870 (88.3) |
408 (84.1) |
106 (87.6) |
965 (80.7) |
<0.001 |
|
Yes |
380 (11.7) |
77 (15.9) |
15 (12.4) |
231 (19.3) |
|
Body mass index (kg/m2) |
25.0±3.1 |
24.7±3.1 |
23.9±2.8 |
23.5±3.1 |
<0.001 |
|
Body temperature (℃) |
36.3±0.4 |
36.3±0.4 |
36.2±0.4 |
36.3±0.4 |
0.009 |
|
Neck circumference (cm) |
36.3±3.2 |
35.4±3.1 |
35.9±3.2 |
34.6±3.1 |
<0.001 |
|
Waist circumference (cm) |
89.0±8.3 |
87.6±8.2 |
86.8±8.7 |
85.2±8.9 |
<0.001 |
|
Sasang Constitution |
Tae-eum |
2,038 (62.7) |
279 (57.5) |
65 (53.7) |
540 (45.2) |
<0.001 |
|
So-eum |
388 (11.9) |
83 (17.1) |
23 (19.0) |
350 (29.3) |
|
So-yang |
824 (25.4) |
123 (25.4) |
33 (27.3) |
306 (25.6) |
2. Comparison of the PSQI scores among the Non-CH, CHF, CHH, and CHHF groups
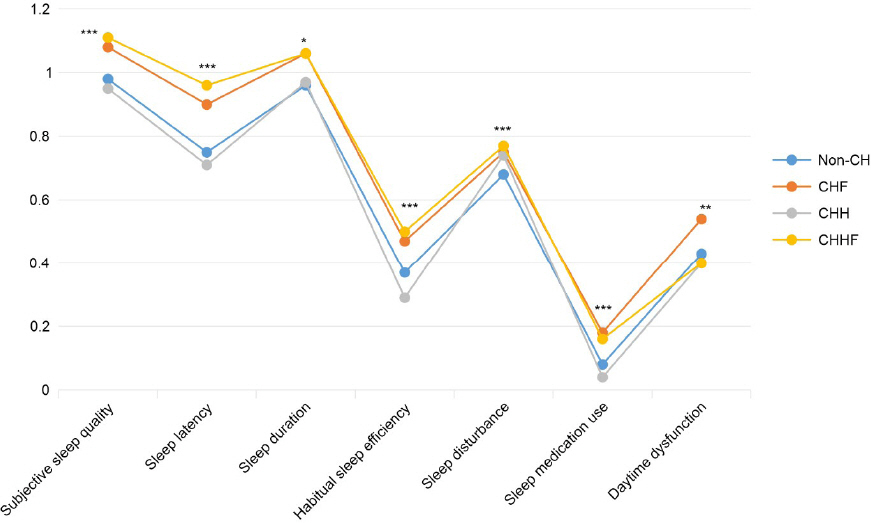
We found significant intergroup differences in the total PSQI scores and in the seven component scores. The total PSQI score and the sub scores, subjective sleep quality, sleep latency, and sleep medication use, were significantly higher in the CHF and CHHF groups than in the Non-CH group (p<0.001); the habitual sleep efficiency and sleep disturbance scores were significantly higher in the CHHF group than in the Non-CH group (p<0.001). Daytime dysfunction scores were significantly higher in the CHF group than in the Non-CH and CHHF groups (p=0.004) ( Table 2, Fig. 2).
Table 2
Comparison of the PSQI among Non-CH, CHF, CHH, and CHHF Groups
|
Non-CH*
|
CHF†
|
CHH‡
|
CHHF§
|
P value |
Scheffé’s |
|
Total PSQI Score |
4.25±3.00 |
4.98±3.47 |
4.11±3.25 |
4.95±3.48 |
<0.001 |
b,d>a |
|
PSQI components |
|
|
|
|
|
|
|
Subjective sleep quality |
0.98±0.65 |
1.08±0.69 |
0.95±0.71 |
1.11±0.71 |
<0.001 |
b,d>a |
|
Sleep latency |
0.75±0.92 |
0.90±0.96 |
0.71±0.87 |
0.96±1.05 |
<0.001 |
b,d>a |
|
Sleep duration |
0.96±0.98 |
1.06±1.01 |
0.97±1.00 |
1.06±1.01 |
0.021 |
|
|
Habitual sleep efficiency |
0.37±0.78 |
0.47±0.91 |
0.29±0.75 |
0.50±0.92 |
<0.001 |
d>a |
|
Sleep disturbance |
0.68±0.61 |
0.75±0.63 |
0.74±0.60 |
0.77±0.64 |
<0.001 |
d>a |
|
Sleep medication use |
0.08±0.43 |
0.18±0.67 |
0.04±0.27 |
0.16±0.64 |
<0.001 |
b,d>a |
|
Daytime dysfunction |
0.43±0.73 |
0.54±0.81 |
0.40±0.67 |
0.40±0.75 |
0.004 |
b>a,d |
|
Poor sleeper |
300 (9.2) |
74 (15.3) |
12 (9.9) |
179 (15.0) |
<0.001 |
|
Fig. 2
The PSQI component scores for the Non-CH, CHF, CHH, and CHHF groups.
P-values were calculated using ANOVA. * : p<0.05, ** : p<0.01, *** : p<0.001. Key : Non-CH : non-cold-hypersensitivity, CHF : cold hypersensitivity in the feet, CHH : cold hypersensitivity in the hands, CHHF : cold hypersensitivity in the hands and feet
The results of the multiple regression analysis to investigate the effects of CH status on PSQI scores are shown in Table 3 (Model 3). Even after correcting for age, sex, BMI, blood pressure, body temperature, neck and waist circumference, and sociodemographic variables, the CHF and CHHF groups showed significantly higher total PSQI scores and significantly different subjective sleep quality, sleep latency, habitual sleep efficiency, sleep disturbance, and sleep medication use. For the sleep duration component, only the CHHF group showed a significantly higher score than the Non-CH group (B=0.09, p=0.011), while the other groups showed no differences. For the daytime dysfunction component, only the CHF group showed a significantly higher score than the Non-CH group (B=0.09, p=0.009).
Table 3
Multiple Regression Analysis for the Association of CH Status and PSQI
|
Model 1 |
Model 2 |
Model 3 |
|
B |
95% CI |
P |
B |
95% CI |
P |
B |
95% CI |
P |
|
Total PSQI score |
|
CHF*
|
0.74 |
0.43-1.04 |
<0.001 |
0.68 |
0.38-0.98 |
<0.001 |
0.72 |
0.42-1.02 |
<0.001 |
|
CHH†
|
-0.14 |
-0.72-0.44 |
0.634 |
-0.13 |
-0.70-0.44 |
0.664 |
-0.11 |
-0.67-0.46 |
0.708 |
|
CHHF‡
|
0.70 |
0.49-0.91 |
<0.001 |
0.52 |
0.30-0.73 |
<0.001 |
0.51 |
0.29-0.72 |
<0.001 |
|
PSQI components : |
|
Subjective sleep quality |
|
CHF*
|
0.10 |
0.04-0.17 |
0.001 |
0.10 |
0.03-0.16 |
0.004 |
0.10 |
0.04-0.16 |
0.002 |
|
CHH†
|
-0.03 |
-0.15-0.09 |
0.638 |
-0.03 |
-0.15-0.09 |
0.629 |
-0.03 |
-0.15-0.09 |
0.671 |
|
CHHF‡
|
0.13 |
0.08-0.17 |
<0.001 |
0.10 |
0.05-0.14 |
<0.001 |
0.09 |
0.05-0.14 |
<0.001 |
|
Sleep latency |
|
CHF*
|
0.15 |
0.06-0.24 |
0.002 |
0.13 |
0.04-0.21 |
0.006 |
0.14 |
0.05-0.23 |
0.002 |
|
CHH†
|
-0.04 |
-0.21-0.13 |
0.655 |
-0.05 |
-0.22-0.12 |
0.577 |
-0.04 |
-0.21-0.13 |
0.660 |
|
CHHF‡
|
0.21 |
0.15-0.28 |
<0.001 |
0.13 |
0.07-0.19 |
<0.001 |
0.13 |
0.06-0.19 |
<0.001 |
|
Sleep duration |
|
CHF*
|
0.09 |
-0.00-0.19 |
0.059 |
0.07 |
-0.03-0.16 |
0.153 |
0.07 |
-0.03-0.16 |
0.182 |
|
CHH†
|
0.00 |
-0.18-0.18 |
0.980 |
0.03 |
-0.15-0.21 |
0.747 |
0.03 |
-0.15-0.21 |
0.741 |
|
CHHF‡
|
0.09 |
0.03-0.16 |
0.006 |
0.09 |
0.02-0.16 |
0.010 |
0.09 |
0.02-0.16 |
0.011 |
|
Habitual sleep efficiency |
|
CHF*
|
0.10 |
0.02-0.18 |
0.014 |
0.10 |
0.02-0.18 |
0.011 |
0.11 |
0.03-0.19 |
0.006 |
|
CHH†
|
-0.08 |
-0.23-0.07 |
0.298 |
-0.07 |
-0.22-0.08 |
0.348 |
-0.07 |
-0.22-0.08 |
0.380 |
|
CHHF‡
|
0.13 |
0.07-0.18 |
<0.001 |
0.11 |
0.05-0.16 |
<0.001 |
0.10 |
0.05-0.16 |
<0.001 |
|
Sleep disturbance |
|
CHF*
|
0.08 |
0.02-0.14 |
0.012 |
0.08 |
0.03-0.14 |
0.005 |
0.10 |
0.04-0.16 |
0.001 |
|
CHH†
|
0.07 |
-0.05-0.18 |
0.257 |
0.06 |
-0.05-0.17 |
0.268 |
0.06 |
-0.04-0.17 |
0.235 |
|
CHHF‡
|
0.09 |
0.05-0.13 |
<0.001 |
0.06 |
0.01-0.10 |
0.009 |
0.05 |
0.01-0.09 |
0.012 |
|
Sleep medication use |
|
CHF*
|
0.11 |
0.06-0.15 |
<0.001 |
0.11 |
0.06-0.16 |
<0.001 |
0.11 |
0.06-0.16 |
<0.001 |
|
CHH†
|
-0.04 |
-0.13-0.06 |
0.441 |
-0.04 |
-0.13-0.05 |
0.413 |
-0.04 |
-0.13-0.05 |
0.404 |
|
CHHF‡
|
0.08 |
0.05-0.12 |
<0.001 |
0.07 |
0.03-0.10 |
<0.001 |
0.07 |
0.03-0.10 |
<0.001 |
|
Daytime dysfunction |
|
CHF*
|
0.12 |
0.04-0.19 |
0.001 |
0.10 |
0.03-0.17 |
0.006 |
0.09 |
0.02-0.16 |
0.009 |
|
CHH†
|
-0.02 |
-0.16-0.11 |
0.740 |
-0.03 |
-0.16-0.10 |
0.669 |
-0.03 |
-0.17-0.10 |
0.624 |
|
CHHF‡
|
-0.03 |
-0.08-0.02 |
0.236 |
-0.02 |
-0.07-0.03 |
0.410 |
-0.02 |
-0.07-0.03 |
0.400 |
3. Differences in the frequencies and odds ratios of poor sleep (PSQI≥8.5) associating with CH status
The ratio of “poor sleepers” (PSQI≥8.5) was 9.2% in the Non-CH group and 9.9% in the CHH group, whereas it was 15.3% in the CHF group and 15.0% in the CHHF group, a significant intergroup difference (p<0.001, Table 2).
Table 4 shows the odds ratios and 95% confidence intervals for “poor sleeper” status in each group, with the Non-CH group as reference. In the unadjusted model (Model 1), when correcting for sex, age, and BMI (Model 2), and when additionally correcting for body temperature, systolic blood pressure, diastolic blood pressure, neck circumference, waist circumference, drinking, smoking, marital status, and education (Model 3), the CHF and CHHF groups showed odds ratios significantly higher than one in all three models (p<0.001), whereas the CHH group did not show any significant differences from the reference group.
Table 4
Odds Ratios and 95% Confidence Intervals for Poor Sleepers (PSQI≥8.5) according to CH Status
|
CHF*
|
CHH†
|
CHHF‡
|
|
Model 1 |
1.77 (1.35-2.33)***
|
1.08 (0.59-1.99) |
1.73 (1.42-2.11)***
|
|
Model 2 |
1.76 (1.33-2.32)***
|
1.14 (0.62-2.11) |
1.54 (1.25-1.90)***
|
|
Model 3 |
1.83 (1.38-2.43)***
|
1.15 (0.62-2.13) |
1.53 (1.25-1.89)***
|
IV. Discussion
In this study, we investigated the relationship between sleep and CH status (in the hands, feet, and hands and feet) in a 5,052-participant cohort study based on two regions in South Korea. There have been relatively few prior studies on CH and sleep compared with studies on the relationship between sleep and other diseases/symptoms. Furthermore, most studies to date have been conducted on limited groups of participants, such as females 9, hospitalized patients 10, or specific age groups 12, making it difficult to generalize the results to the population as a whole. Specifically, there has been no previous study on Korean subjects that examined the relationship between CH (hands, feet, and both hands and feet) and PSQI scores. We believe that our findings, when combined with the existing literature, help elucidate and generalize the relationship between sleep and CH. The mean age of the 5,052 participants was 62 years, with 4% more women than men. However, 35.7% of the participants had CH. This is similar to a previous report of a nationwide questionnaire survey of 2,201 adults selected using stratified multistage sampling to be representative of the Korean population, which found a CH prevalence of 34.2% 14. The distribution of Sasang constitutional types differed between the groups. In the non-CH group, the Taeeum-in type was the most prevalent at 62.7%, while in the CHHF group, it was relatively lower at 45.2%. Conversely, the Soeum-in type was more prevalent in the CHHF group at 29.3%, compared to 11.9% in the non-CH group. These results are similar to a previous study that reported a higher cold sensation score in the hands and feet of the Soeum-in group compared to the Taeeum-in group 26. In the present study, we analyzed the relationship between CH and PSQI by using correlation and multiple regression analyses, as shown in Supplementary Tables 1 and 2, not only with CH but also with various variables known to be related. Through this, we found that having a spouse and higher education were positively related to sleep quality, whereas CHHF, CHF, female gender, and age were negatively related. We then discovered that when sleep scores were stratified by CH status, the total PSQI score was higher in the CHF and CHHF groups than in the Non-CH group. This is similar to the results of a study of 238 Japanese women, in which the cold-extremities group showed higher PSQI scores than did the Non-cold-extremities group 9. Interestingly, in the present study, the CHH group did not show any differences from the Non-CH group. The ratio of “poor sleepers” was 15.3% and 15.0% in the CHF and CHHF groups, respectively, which differed by approximately 6% from that of the Non-CH group (9.2%), whereas the CHH group (9.9%) did not show any significant differences. Given that 63% of participants in a study of people with primary vasospastic syndrome reported cold feet as a reason for sleep-onset difficulties 18, CHF seems to be a more important cause and accompanying symptom of poor sleep quality than does CHH. Several previous studies on sleep and cold extremities have reported that cold extremities are strongly related to prolonged sleep-onset latency 12,27,28. Immediately before sleep onset, the core temperature of the body drops due to the heat of the body moving from the center to the hands and feet, due to vasodilation in the periphery, which results in rapid heat loss. However, people with cold extremities do not show a normal peripheral vasodilation response, which produces symptoms such as prolonged sleep-onset latency and difficulty in initiating sleep 27,29. In the present study, even when correcting for other variables, the sleep-onset latency component of the PSQI showed higher scores in the CHF and CHHF groups. Moreover, most other component scores were also significantly higher in the CHF and CHHF groups. This suggests that sleep latency was extended due to cold extremities, which then affected other components (e.g., subjective sleep, habitual sleep efficiency, or sleep medication). However, given that the sleep disturbance scores were also higher in these groups, cold extremities appear to play a role in interfering with not only sleep onset but also with sleep maintenance. Cold extremities are common in the population, even in people without disease. Although the pathological mechanism has not been clearly elucidated, it is thought to involve autonomic nerve malfunction (especially a higher adrenergic sensitivity for vasoconstriction in the distal portion of the extremities) and problems in the vascular endothelial cells 15,16,30. In Western medicine, the presence of cold extremities is not considered to require treatment by itself, but in traditional East Asian medicine, cold extremities are considered a root cause of several diseases (a type of constitution), thus requiring treatment 10,12. Such differences in opinion notwithstanding, studies from several countries have reported that patients with this condition are predisposed to dyspepsia, chronic rhinitis, reflux esophagitis, hypotension, normal-tension glaucoma, migraine, fatigue, and menstrual pain, while showing lower rates of diabetes, arteriosclerosis, and dyslipidemia 16,24,31,32. Patients may present with different types of sleep disorders depending on whether they have cold extremities. Moreover, even if they have the same type of sleep disorder (or symptoms), different pathological mechanisms may be involved in the presence or absence of cold extremities. For instance, obese individuals who report less cold extremities tend to be susceptible to obstructive sleep apnea syndrome, while those with cold extremities are known to experience prolonged sleep latency or relatively shorter total sleep time, including REM sleep 18,33,34. Taken together, these facts suggest that differentiation of patients’ characteristics is an important factor in overcoming sleep disorders. Examples of such differentiation are the pattern identification and constitutional approaches of traditional East Asian medicine 35,36. The perspective of Korean medicine on sleep disorders varies depending on the type of disorder. In cases of hypersomnia, sleep and wakefulness are associated with the circulation of wei-qi (衛氣), prioritizing the pathology of yang deficiency (陽虛) over yin deficiency (陰虛). Conversely, in cases of insomnia, the pathologies of yin deficiency (陰虛) or liver fire (肝火) are more prevalent 37. One diagnostic element for these syndromes is the presence of excessive heat or cold sensations in the body. A study reported that individuals experiencing both heat and cold sensations had a higher degree of insomnia 38. As analyzed in this study, CHHF can negatively impact overall sleep quality, including sleep latency and sleep disturbance. Although CHHF is primarily observed in yang deficiency (陽虛), it can also be seen in heat syndromes (熱證) such as heat syncope (熱厥) 39. Therefore, a comprehensive diagnosis based on syndrome differentiation is essential in treating patients with sleep disorders. There is no clear evidence that improving CHHF directly improves sleep disorders or that improving sleep disorders alleviates CHHF. However, there is a case report where prescribing Oryeong-san (五苓散) to insomnia patients with CHHF led to improvement 40. Additionally, a meta-analysis reported that treatments including Sayeok-san (四逆散), a representative prescription for treating CHHF, were more effective in improving insomnia compared to Western medicine alone 41. These reports support this possibility. This study has several limitations. First, although we analyzed cohort data, this was a cross-sectional study. Therefore, we were only able to investigate the association between CH status and sleep quality and were not able to identify a causal relationship. Second, because CH and sleep quality were both assessed using self-report questionnaires, we cannot exclude the possibility of bias. Third, apart from the mechanism related to delayed sleep-onset latency that we have discussed ,24,26 we did not determine how cold extremities may increase the scores of the PSQI components (i.e., the mechanisms linking cold extremities to poor sleep quality). Fourth, the data used in this study was collected between 2012 and 2015, which may limit the ability of the research findings to fully reflect the current reality due to potential changes in the BMI or weight of the Korean population over time. In conclusion, we confirmed that CH of the feet (CHF and CHHF) was associated with poor sleep quality. We believe that our findings will help to elucidate the relationship between sleep and CH. Importantly, these results can provide evidence supporting the use of pattern identification in diagnosing and treating sleep disorders in Korean medicine. Further studies to investigate the causal relationship and underlying mechanisms are warranted.
Acknowledgments
This study was supported by grants from the Korea Institute of Oriental Medicine (Grant No. KSN1732121).
References
1. Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch 2012:463(1):121–37.   2. Harding EC, Franks NP, Wisden W. Sleep and thermoregulation. Curr Opin Physiol 2020:15:7–13.  3. Shokri-Kojori E, Wang GJ, Wiers CE, Demiral SB, Guo M, Kim SW, et al. β-Amyloid accumulation in the human brain after one night of sleep deprivation. Proc Natl Acad Sci USA 2018:115(17):4483–8. 4. Singareddy R, Vgontzas AN, Fernandez-Mendoza J, Liao D, Calhoun S, Shaffer ML, et al. Risk factors for incident chronic insomnia:a general population prospective study. Sleep Med 2012:13(4):346–53. 5. Uhlig BL, Sand T, Odegård SS, Hagen K. Prevalence and associated factors of DSM-V insomnia in Norway:the Nord-Trøndelag Health Study (HUNT 3). Sleep Med 2014:15(6):708–13. 6. Kim KW, Kang SH, Yoon IY, Lee SD, Ju GW, Han JW, et al. Prevalence and clinical characteristics of insomnia and its subtypes in the Korean elderly. Arch Gerontol Geriatr 2017:68:68–75. 8. Wolkove N, Elkholy O, Baltzan M, Palayew M. Sleep and aging:1. Sleep disorders commonly found in older people. CMAJ 2007:176(9):1299–304. 9. Tsuboi S, Mine T, Tomioka Y, Shiraishi S, Fukushima F, Ikaga T. Are cold extremities an issue in women's health?Epidemiological evaluation of cold extremities among Japanese women. Int J Womens Health 2019:11:31–9. 11. Phillips B, Mannino D. Correlates of sleep complaints in adults:the ARIC study. J Clin Sleep Med 2005:1(3):277–83. 12. Krauchi K, Gasio PF, Vollenweider S, Von Arb M, Dubler B, Orgül S, et al. Cold extremities and difficulties initiating sleep:evidence of co-morbidity from a random sample of a Swiss urban population. J Sleep Res 2008:17(4):420–6. 13. Hur YM, Chae JH, Chung KW, Kim JJ, Jeong HU, Kim JW, et al. Feeling of cold hands and feet is a highly heritable phenotype. Twin Res Hum Genet 2012:15(2):166–9. 16. Konieczka K, Ritch R, Traverso CE, Kim DM, Kook MS, Gallino A, et al. Flammer syndrome. EPMA J 2014:5(1):11. 17. Na ID, Park MS, Kim YM. The study on Korean medical pattern differentiation of sleep-wake disorders by DSM-V classification. J Physiol &Pathol Korean Med 2017:31(2):83–93.
18. Pache M, Kräuchi K, Cajochen C, Wirz-Justice A, Dubler B, Flammer J, et al. Cold feet and prolonged sleep-onset latency in vasospastic syndrome. Lancet 2001:358(9276):125–6. 19. Kim YJ, Han BG. KoGES group. Cohort profile:The Korean Genome and Epidemiology Study (KoGES) Consortium. Int J Epidemiol 2017:46(2):e20. 21. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index:a new instrument for psychiatric practice and research. Psychiatry Res 1989:28(2):193–213. 22. Sohn SI, Kim DH, Lee MY, Cho YW. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath 2012:16(3):803–12.  23. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003:42(6):1206–52. 25. Bae KH, Kim SH, Go HY, Park KH, Lee SW, Lee SJ. One year test-retest reliability of the Korea Sasang constitutional diagnostic questionnaire (KS-15) in university students. J Sasang Constitut Med 2019:31(2):12–21.
26. Bae KH, Park KH, Lee SW. Cold hypersensitivity in the Hands, Feet and Abdomen according to Sasang Constitution. J Sasang Constitut Med 2018:30(1):50–7.
27. Kräuchi K, Cajochen C, Werth E, Wirz-Justice A. Warm feet promote the rapid onset of sleep. Nature 1999:401(6748):36–7. 28. Vollenweider S, Wirz-Justice A, Flammer J, Orgül S, Kräuchi K. Chronobiological characterization of women with primary vasospastic syndrome:body heat loss capacity in relation to sleep initiation and phase of entrainment. Am J Physiol Regul Integr Comp Physiol 2008:294(2):R630–8. 29. Kräuchi K. The thermophysiological cascade leading to sleep initiation in relation to phase of entrainment. Sleep Med Rev 2007:11(6):439–51. 33. Bae KH, Park KH, Ahn IK, Lim SE, Lee S. Cold Feet and Sleep Quality :An Exploratory Study Using Polysomnography and Pittsburgh Sleep Quality Index. Journal of Society of Preventive Korean Medicine 2024:28(1):109–18.
34. Resta O, Foschino-Barbaro MP, Legari G, Talamo S, Bonfitto P, Palumbo A, et al. Sleep-related breathing disorders, loud snoring and excessive daytime sleepiness in obese subjects. Int J Obes Relat Metab Disord 2001:25(5):669–75. 35. Yang JL, Zhang R, Du L, Yang YS, Liu XC. Clinical observation on the neurotransmitters regulation in patients of insomnia differentiated as yang deficiency pattern treated with warm acupuncture and auricular point sticking therapy. Zhongguo Zhen Jiu 2014:34(12):1165–8. 37. Na ID, Park MS, Kim YM. The study on Korean medical pattern differentiation of sleep-wake disorders by DSM-V classification. J Physiol &Pathol Korean Med 2017:31(2):83–93.
38. Mun SJ, Park KH, Bae KH, Baek YH, Lee SW. Association of cold/heat sensation with sleep quality and insomnia in middle-aged women. J Korean Med 2024:45(1):125–36. 39. Huh TY, Ha DJ, Kim KM. The Effect of Sayeok-san for Insomnia:A Systematic Review and Meta-Analysis. J Int Korean Med 2021:42(4):547–62. 40. Park JK. A Case Report of Primary Insomnia treated by Oryeong-san decoction. J of KMediACS 2015:7(1):45–52.
41. Huh TY, Ha DJ, Kim KM. The Effect of Sayeok-san for Insomnia:A Systematic Review and Meta-Analysis. J Int Korean Med 2021:42(4):547–62.
【Supplementary】
Table 1
Correlation between Observed PSQI Score and Covariates
|
PSQI Total |
CHH |
CHF |
Alcohol |
Tobacco |
SBP |
DBP |
BMI |
Gender |
Age |
Education |
Marital status |
Body temperature |
Neck circumference |
Waist circumference |
|
PSQI Total |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHH |
.077**
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHF |
.108**
|
.754**
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Alcohol |
-.045**
|
-.059**
|
-.065**
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
Tobacco |
-.048**
|
-.030*
|
-.060**
|
.259**
|
1 |
|
|
|
|
|
|
|
|
|
|
|
SBP |
.046**
|
-.079**
|
-.086**
|
0.015 |
-0.002 |
1 |
|
|
|
|
|
|
|
|
|
|
DBP |
-0.007 |
-.087**
|
-.076**
|
.134**
|
.051**
|
.665**
|
1 |
|
|
|
|
|
|
|
|
|
BMI |
-0.017 |
-.236**
|
-.196**
|
0.006 |
-.084**
|
.184**
|
.216**
|
1 |
|
|
|
|
|
|
|
|
Gender |
.136**
|
.118**
|
.155**
|
-.454**
|
-.374**
|
-.037**
|
-.147**
|
.035*
|
1 |
|
|
|
|
|
|
|
Age |
.114**
|
0.014 |
-.039**
|
-.199**
|
-.110**
|
.291**
|
-.069**
|
-.039**
|
.068**
|
1 |
|
|
|
|
|
|
Education |
-.135**
|
-.040**
|
0.005 |
.211**
|
.124**
|
-.218**
|
-0.015 |
-.036*
|
-.314**
|
-.472**
|
1 |
|
|
|
|
|
Marital status |
-.101**
|
-0.02 |
-0.028 |
.145**
|
.064**
|
-.083**
|
0.01 |
-0.009 |
-.249**
|
-.240**
|
.212**
|
1 |
|
|
|
|
Body temperature |
-0.005 |
-0.003 |
0.023 |
-.100**
|
-.137**
|
-.096**
|
-.079**
|
.061**
|
.259**
|
-.090**
|
.047**
|
-0.017 |
1 |
|
|
|
Neck circumference |
-.090**
|
-.202**
|
-.207**
|
.350**
|
.252**
|
.160**
|
.253**
|
.459**
|
-.726**
|
-.080**
|
.211**
|
.175**
|
-.192**
|
1 |
|
|
Waist circumference |
.028*
|
-.202**
|
-.186**
|
0.027 |
-0.025 |
.267**
|
.239**
|
.830**
|
-.064**
|
.133**
|
-.126**
|
-.031*
|
-.029*
|
.529**
|
1 |
Table 2
Odds Ratios and 95% Confidence Intervals for Poor Sleepers (PSQI≥8.5)
|
Variable |
OR |
95% Confidence Interval |
p value |
|
Model 1 |
CH group |
|
|
|
|
Non-CH*
|
1 |
|
|
|
CHF†
|
1.77 |
1.35-2.33 |
<0.001 |
|
CHH‡
|
1.08 |
0.59-1.99 |
0.798 |
|
CHHF§
|
1.73 |
1.42-2.11 |
<0.001 |
|
Model 2 |
CH group |
|
|
|
|
Non-CH*
|
1 |
|
|
|
CHF†
|
1.76 |
1.33-2.32 |
<0.001 |
|
CHH‡
|
1.14 |
0.62-2.11 |
0.670 |
|
CHHF§
|
1.54 |
1.25-1.90 |
<0.001 |
|
Gender |
|
|
|
|
Male |
1 |
|
|
|
Female |
1.88 |
1.55-2.28 |
<0.001 |
|
Age |
1.04 |
1.03-1.05 |
<0.001 |
|
Body mass index |
1.00 |
0.97-1.03 |
0.847 |
|
Model 3 |
CH group |
|
|
|
|
Non-CH*
|
|
|
|
|
CHF†
|
1.83 |
1.38-2.43 |
<0.001 |
|
CHH‡
|
1.15 |
0.62-2.13 |
0.661 |
|
CHHF§
|
1.53 |
1.25-1.89 |
<0.001 |
|
Gender |
|
|
|
|
Male |
|
|
|
|
Female |
2.01 |
1.41-2.86 |
<0.001 |
|
Age |
1.02 |
1.01-1.04 |
<0.001 |
|
Body mass index |
0.96 |
0.91-1.01 |
0.127 |
|
Body temperature |
0.93 |
0.72-1.22 |
0.604 |
|
Systolic blood pressure |
1.00 |
0.99-1.01 |
0.638 |
|
Diastolic blood pressure |
1.00 |
0.99-1.01 |
0.948 |
|
Neck circumference |
1.03 |
0.97-1.09 |
0.390 |
|
Waist circumference |
1.01 |
0.99-1.03 |
0.192 |
|
Alcohol |
|
|
|
|
No |
1 |
|
|
|
Yes |
1.23 |
1.00-1.52 |
0.052 |
|
Tobacco |
|
|
|
|
No |
1 |
|
|
|
Yes |
1.01 |
0.73-1.40 |
0.940 |
|
Marital status |
|
|
|
|
Spouseless |
1 |
|
|
|
Married |
0.69 |
0.55-0.87 |
0.002 |
|
Education |
|
|
|
|
Elementary |
1 |
|
|
|
Middle, High |
0.74 |
0.60-0.93 |
0.008 |
|
≥College |
0.56 |
0.39-0.82 |
0.002 |
|
|